Detail
Source:https://pubs.acs.org/doi/10.1021/acs.jmedchem.0
Abstract
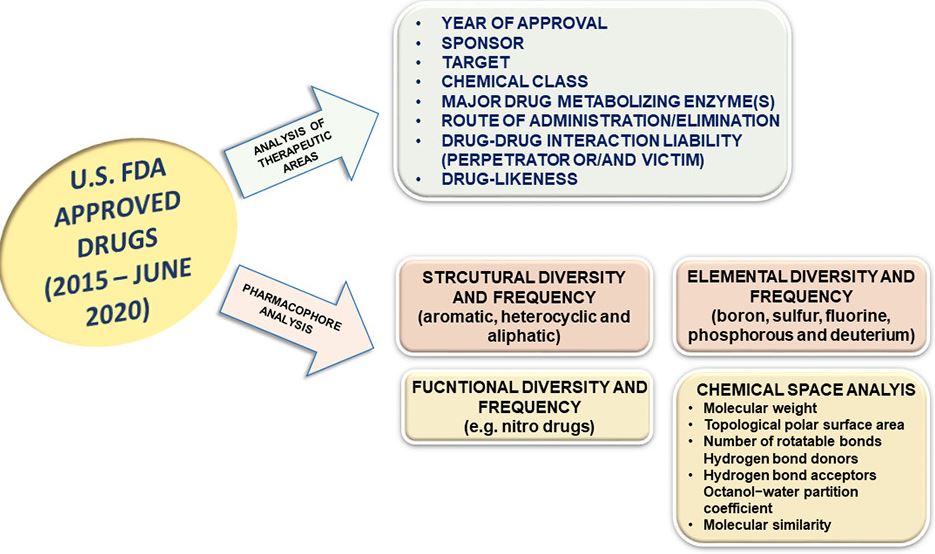
In the present work, we report compilation and analysis of 245 drugs, including small and macromolecules approved by the U.S. FDA from 2015 until June 2020. Nearly 29% of the drugs were approved for the treatment of various types of cancers. Other major therapeutic areas of focus were infectious diseases (14%); neurological conditions (12%); and genetic, metabolic, and cardiovascular disorders (7–8% each). Itemization of the approved drugs according to the year of approval, sponsor, target, chemical class, major drug-metabolizing enzyme(s), route of administration/elimination, and drug–drug interaction liability (perpetrator or/and victim) is presented and discussed. An effort has been made to analyze the pharmacophores to identify the structural (e.g., aromatic, heterocycle, and aliphatic), elemental (e.g., boron, sulfur, fluorine, phosphorus, and deuterium), and functional group (e.g., nitro drugs) diversity among the approved drugs. Further, descriptor-based chemical space analysis of FDA approved drugs and several strategies utilized for optimizing metabolism leading to their discoveries have been emphasized. Finally, an analysis of drug-likeness for the approved drugs is presented.
Introduction
Drug discovery is a complex interdisciplinary process, and it continues to pose a plethora of challenges for the pharmaceutical industry and allied fields.(1) In recent times, the expectations from new drugs to exhibit better performance over the existing ones in the market has increased tremendously.(2) The main reason attributed to this is probably the strict requirements imposed by different regulatory agencies around the world.(3,4) Considering the last five years of approvals (2015–June 2020) by the Centre for Drug Evaluation and Research (CDER) of the U.S. FDA, a total of 245 drugs were approved including small and macromolecules (Figure 1). Of these, a record number of drugs were approved in 2018 (59), and a minimum of approvals came through in 2016 (22). For all the other years of the study (i.e., 2015, 2017, and 2019), the number of new drug approvals from the agency remained in the range of 45–48. Approval of 25 drugs until June 2020 indicates that this year also might end up with a similar number of approvals.(5−7) Among the different therapeutic categories, anticancer drugs accounted for 29% of drug approvals followed by anti-infectives (14%) and drugs for neurological disorders (12%). Other major areas of focus from the pharmaceutical industry wherein approvals came through were genetic, autoimmune, cardiac, and metabolic disorders (each ranging between 6 and 8%).
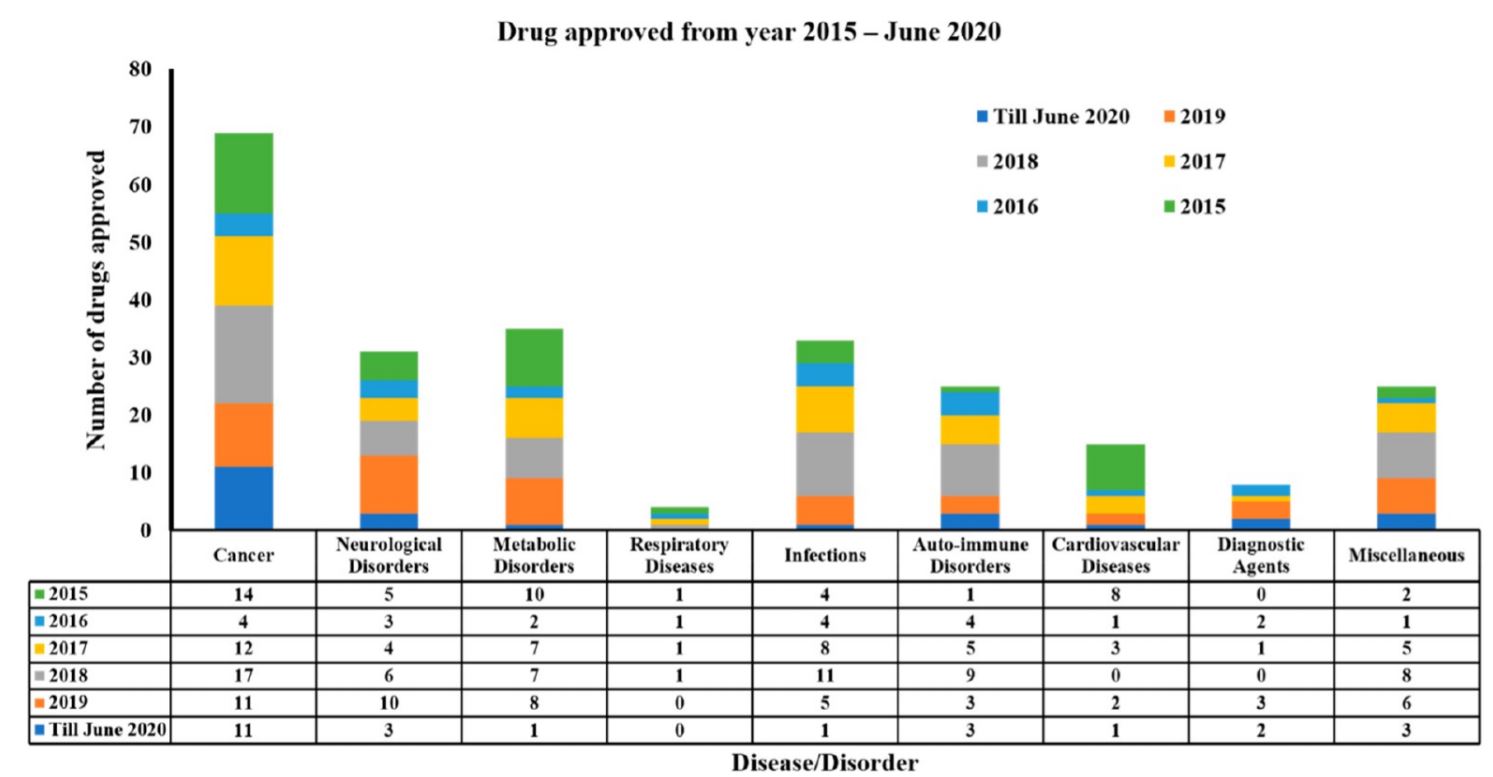
Figure 1. Bar graph illustration of the number of year-wise drug approvals for various diseases/disorders. The data pertains to 2015–June 2020. The source of the data is the U.S. FDA Web site(8) and DrugBank database.(9)
Considering the drug discovery, on an average, one drug out of every 8000–10 000 compounds is approved for the market.(10) The drug-likeness for any compound is largely determined by its pharmacokinetics (PK), safety, and efficacy. The goal of PK studies is to ascertain and eventually help achieve the desired efficacy and safety profile.(11−13) Efficacy, safety, and PK are interconnected, and assigning the cause of failure of a compound to any one of these factors could be misleading. For example, extensive metabolism could be one of the reasons for not achieving the desired efficacy, and toxicity might be observed because of the formation of metabolites.(14) The benzylic C–H bond and the allylic methyl and O-, N-, S-methyl groups, when not sterically hindered, are ideal metabolic soft spots and substrates of cytochrome (CYP) P450 mediated oxidative and reductive metabolism reactions. Overall, CYP enzymes are responsible for the metabolism of most of the small molecules. However, the structure–metabolism relationship of drugs metabolized through CYPs is complex. Hydrophobic, steric, hydrogen bonding, or ionic interactions with specific amino acids at the active site of the enzyme determine the affinity of the substrate with the active site of an enzyme. Common methods to decrease and/or block metabolism are (1) replacing the H atom of the C–H bond with a bulky group, bioisostere, a deuterium, or a halogen atom; or (2) place a bulky group in a neighboring site to decrease or block the accessibility of the enzyme. For example, when a benzylic methyl group is identified as a metabolic soft spot, a halogen atom, or a −CF3 group, could be used to replace the H atom of the benzylic methyl group.
An ideal drug candidate should be able to provide sustained exposure to have increased patient compliance due to decreased dosing frequency. It should undergo balanced clearance pathways and should not interfere with DMEs (drug-metabolizing enzymes) and transporters. In general, drugs are classified as either victims (directly affected) or perpetrators (cause interactions) in DDI (drug–drug interactions).(15) Medicinal chemists optimizing their compounds for candidate selection are often posed with the following questions: (1) What is the elimination pathway for the molecule of interest? (2) What are the metabolic liabilities of the molecule? (3) Does the compound of interest have the chance to undergo bioactivation to form a reactive metabolite? (4) Do any of the metabolites have either on- or off-target activity?(16) Two other essential parameters controlling rate and extent of absorption of drugs are solubility and permeability, and a Biopharmaceutics Classification System (BCS) for correlating in vitro dissolution and in vivo bioavailability has been proposed.(17) Several theories are available on predicting the “requisite” physicochemical properties for “drug-like” absorption potential for new chemical entities. As per Lipinski’s rule, reduced intestinal permeability is reported for compounds (intended to be administered orally) with more than two out-of-range parameters from the following: more than five hydrogen-bond donors (sum of OH and NH groups), more than 10 hydrogen-bond acceptors (sum of N and O), molecular weight (MW) > 500, and log P > 5.(18−20)
While compiling this Perspective, we came across many worthy reviews on FDA approved drugs which are either yearly publications focusing on a particular issue(6,7,21,22) or are relatively old.(23) In this Perspective, we broadly categorized and discussed in the first section the U.S. FDA approved drug candidates of the last five years (2015–June 2020) based on their therapeutic areas, year of approval, sponsor, target, chemical class (small and macromolecules including antibody–drug conjugates), major drug-metabolizing enzyme(s), route of administration/elimination, and DDI liability (perpetrator and victim). The data was collected from the U.S. FDA Web site and the DrugBank database. In a later section, we comprehensively analyzed the structural (e.g., aromatic, heterocycle, and aliphatic), elemental (e.g., boron, sulfur, fluorine, phosphorus and deuterium), and functional (e.g., nitro drugs) diversity and frequency, and chemical space among the approved drugs and finally pharmacokinetic aspects and market outlook are discussed.
Anti-Cancer Drugs
According to the WHO, more than 100 types of cancer are currently known, and the five most common cancers in 2018 were lung, colorectal, stomach, breast, and liver.(24) Total deaths due to various types of cancer were more than 9 million in that year. Each cancer type requires a separate diagnosis and treatment strategy, which further creates an additional burden on and challenge for the discovery of anticancer drugs. Since the advent of the first anticancer therapy in the 1940s using nitrogen mustards and antifolate drugs,(25) there has been an incredible improvement in the design of new anticancer drugs.(26) The last five years have witnessed the FDA approving a total of 69 drug/drug combinations for the treatment of various types of cancers including 51 small molecules and 19 macromolecules.
Table 1. Illustrative Compilation of U.S. FDA Approved Anti-Cancer Drugs (Small Molecules) from the Year 2015 until June 2020, Featuring Their Indication, Year of Approval, Sponsor, Target, Chemical Class, Major Drug Metabolizing Enzyme(s), Route of Administration/Elimination, and Drug Interactions (Perpetrator or/and Victim)
Figure 2
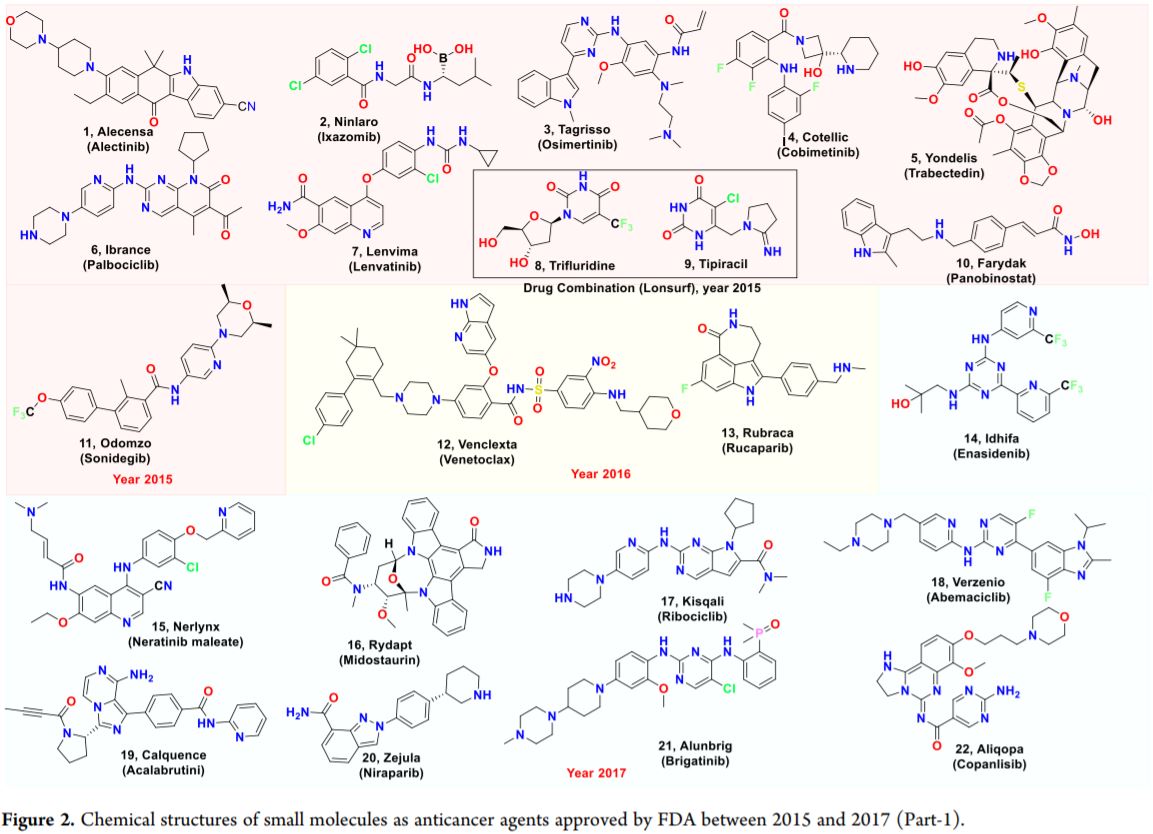
Figure 3
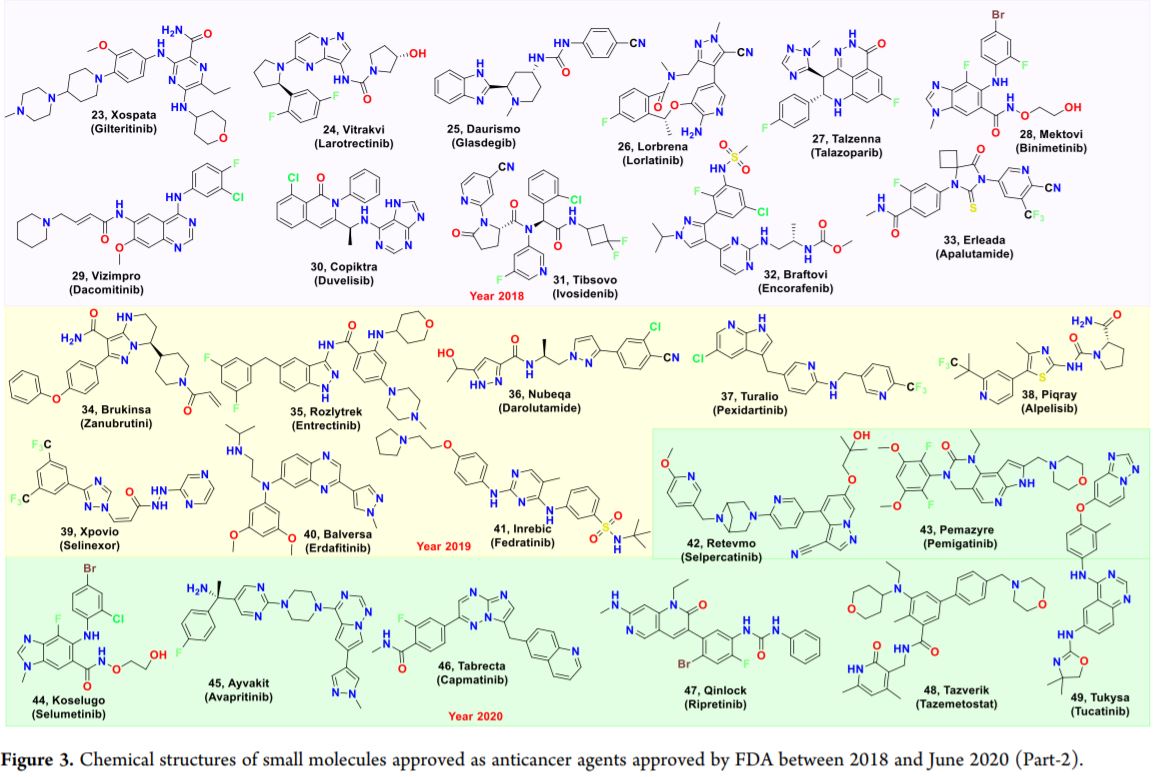
Neratinib (15), a kinase inhibitor, was approved for the treatment of HER2-overexpressed/amplified breast cancer. The other approved anticancer kinase inhibitor drugs included cobimetinib (4), copanlisib (22), and acalabrutib (19) as inhibitors of MAPK, PI3K/AKT, and BTK, respectively. Drugs targeting vascular endothelial growth factor (VEGF; lenvatinib, 7 and brolucizumab), basic fibroblast growth factor (bFGF; erdafitinib, 40 and pemigatinib, 43), platelet-derived endothelial growth factor (PDGFR; olaratumab), and granulocyte colony-stimulating factor (CSF; pexidartinib, 37) were approved in the study period to prevent the formation of new blood vessels and thus subsequently suppress tumor growth. There was one antiapoptotic drug; venetoclax (12) targeting Bcl-2 was approved in the year 2017(27) for the treatment of chronic lymphocytic leukemia. The agency approved first-in-class enasidenib (14), an inhibitor of mutated isocitrate dehydrogenase 2 (IDH2) for acute myeloid leukemia, confirming metabolism-altering drugs as a means of targeting and killing cancer cells. The agency also approved Amgen’s talimogene laherparepvec, the first cancer-killing virus. Several monoclonal antibodies (mAbs) including but not limited to atezolizumab, avelumab, durvalumab, and cemiplimab targeting PD-L1 (immune checkpoints) were approved in the last five years. The approvals also include other immunotherapies and chimeric antigen receptor therapies.(28)
We noticed increased approvals for antibody–drug conjugates (ADCs) since 2015.(29) ADCs are highly selective and allow specific delivery of cytotoxic agents to the intended cancer cell target.(30,31) Their success has been marked by FDA approval of five ADCs in the last five years including inotuzumab ozogamicin for acute lymphoblastic leukemia, fam-trastuzumab deruxtecan for metastatic breast cancer, enfortumab vedotin for refractory bladder cancer, sacituzumab govitecan for metastatic triple-negative breast cancer, and polatuzumab vedotin for relapsed or refractory diffuse large B-cell lymphoma.
Typically, anticancer drugs are coadministered with other drugs and therefore have a high propensity to undergo DDI either as victim and/or perpetrator. Some of the drugs used for cancer therapy act as a victim in the presence of CYP3A4 modulators (both inhibitor as well as inducer) and P-gp (P-glycoprotein) and BCRP (breast cancer resistance protein) inhibitors, while others may be a perpetrator (impact the systemic exposure of coadministered drugs through inhibition of various enzymes like CYP3A4, CYP2C9. CYP2D6, CYP2C19 and transporters like P-gp, BCRP, OATP1B1; see Tables 1 and 2). Overall, CYPs played a significant role in the metabolism of 43 out of 51 small molecules, and for almost all the drugs (42 out of 43), the major enzyme involved is CYP3A4. Rucaparib (13), a first-in-class PARP inhibitor, is metabolized primarily by CYP2D6. Carboxylesterase-mediated amide hydrolysis is the major pathway for the metabolism of niraparib (20), leading to the formation of an inactive acid metabolite followed by glucuronidation. Aldehyde oxidase (AO) along with CYP3A4 are involved in the metabolism of capmatinib (46) and 7 (quinoline derivatives). Catabolism is primarily responsible for the elimination of all the macromolecules. A total of 47 out of 51 anticancer small-molecule drugs were approved for administration through the peroral route and 4 (trabectedin (5), copanlisib (22), lurbinectedin, and lutetium Lu 177 dotatate) through the intravenous route, and all the macromolecules were approved for use through the intravenous route.
Drug design for anticancer drugs has shifted from traditional cytotoxic chemotherapy to targeted cancer drugs,(32) which is further supported with increased understanding of the disease at the molecular level.(33,34) The overall success rate for the oncology drugs in the clinical development is estimated at ∼10%, while the cost of introducing a new drug to the market is estimated at greater than 1 billion US$.(35−37) Unfortunately, the major challenge is the development of drug resistance that leads to mortality and morbidity.(38) Considering the global market, it is anticipated that the targeted anticancer therapy would acquire the highest revenue contribution in cancer drug market by 2026. It is also anticipated that five regions (i.e., North America, Latin America, Europe, Asia Pacific excluding Japan, Middle East, and Africa) would drive anticancer research. AbbVie, Bayer, Pfizer, Bristol Myers Squibb, Roche, Eli Lilly, Novartis, AstraZeneca, and Johnson & Johnson will continue to be major players in the area and would contribute toward more than 2/3rd market share of anticancer drugs.(39)
Drugs for Neurological Disorders
Neurological disorders can be classified into three groups: neurotraumatic diseases (strokes and epilepsy), neurodegenerative diseases including Alzheimer’s disease (AD), Parkinson’s disease (PD), and neuropsychiatric diseases (depression, schizophrenia).(40) Neurological disorders are reported to contribute 11.6% of global disability adjusted life years (DALYs) and 16.5% (2nd leading cause) of deaths from all causes.(41)
Until 2015, there were 79 FDA approved new molecular entities for the treatment of neurological disorders.(42) Over the past five years, FDA has approved a total of 23 small molecules, one each of cyclodextrin derivative and toxin; two oligonucleotides and four monoclonal antibodies for the treatment of neurological disorders. Chemical structures of small molecules approved for the treatment of various neurological disorders are collated in Figure 4.
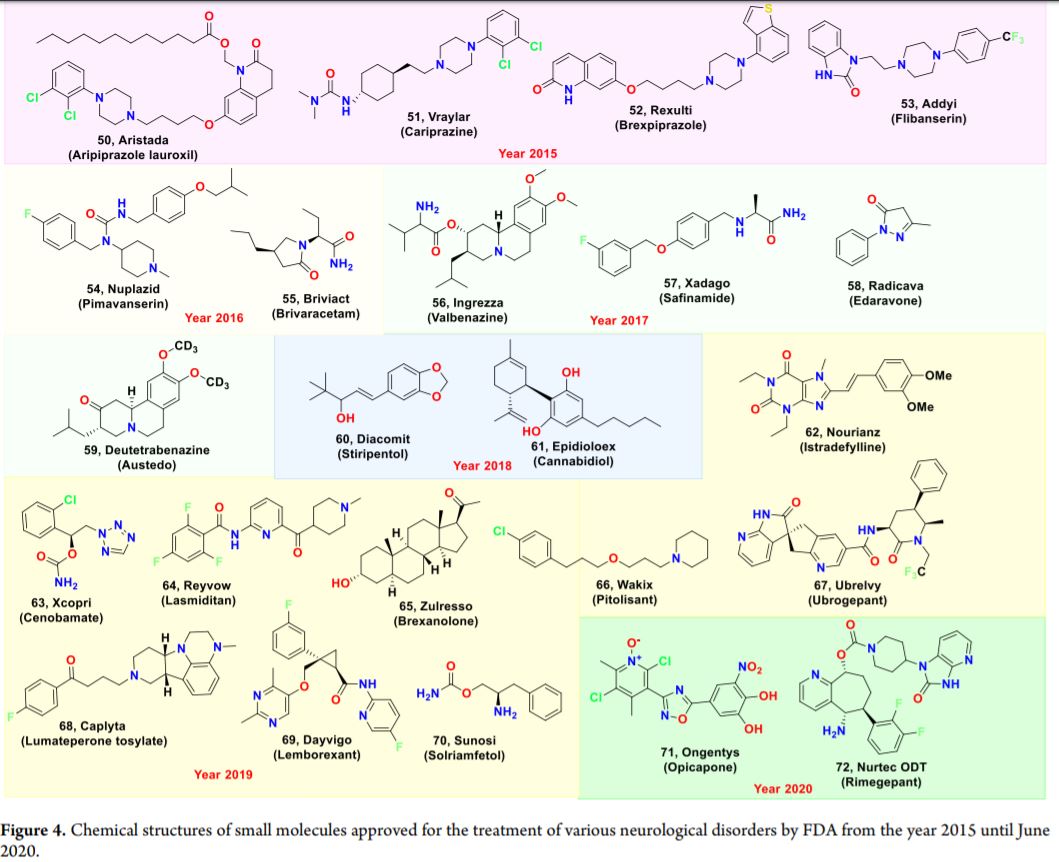
It is evident that serotonin (5-HT1F) and calcitonin gene-related peptide (CGRP) targets were explored for the management of migraine in the last five years. Lasmiditan, (64), a 5-HT1F receptor agonist, exerts effects by inhibition of trigeminal nerve firing and hyperpolarization of nerve terminals.(43) Calcitonin gene-related peptide (CGRP) release produces local vasodilation and extravasation of plasma and plasma proteins into the surrounding tissue.(44) A total of six CGRP antagonists containing two small molecules, ubrogepant (67) and rimegepant sulfate (72), and four monoclonal antibodies, namely, erenumab, fremanezumab, galcanezumab, and eptinezumab, were approved. Further, to circumvent the extrapyramidal motor side effects (EPS) due to full inhibition of dopamine D2 receptors by first-generation antipsychotics, four small molecules with serotonin 5-HT2A receptor antagonism in combination with D2 receptor partial agonism were approved by the FDA for the treatment of schizophrenia. In the antiepileptic category, targets such as gamma-aminobutyric acid (GABA) receptors and synaptic vesicle glycoprotein 2 (SV2) were explored by pharmaceutical companies in the last five years. Cannabidiol (61), an oral solution, was approved in 2018 for the treatment of Dravet syndrome and Lennox-Gastaut syndrome. According to the FDA, 61 does not appear to exert its anticonvulsant effects through interaction with cannabinoid receptors.(45) GABA which acts through GABAA and GABAB receptors is the principal inhibitory neurotransmitter in the brain.(46) Stiripentol (60) and cenobamate (63), positive allosteric modulators of GABAA receptors, were approved in 2018 and 2019, respectively, for the treatment of epilepsy. Brivaracetam (55), which binds SV2A with high affinity and thus induces indirect modulation of synaptic GABA release, was approved in 2016 for the treatment of partial-onset seizures. For the treatment of patients of Parkinson’s disease experiencing “off” episodes, safinamide (57), a reversible inhibitor of MAO-B, and opicapone (71), a third-generation inhibitor of COMT, were approved as an add-on treatment to levodopa(47) and as an adjunctive therapy, respectively. Istradefylline (62), an A2A receptor inhibitor, was approved in 2019 for the treatment of Parkinson’s disease as an adjunct to levodopa therapy. Edaravone (58), a free radical scavenger which increases prostacyclin production and decreases lipoxygenase metabolism of arachidonic acid, was approved for the treatment of amyotrophic lateral sclerosis (ALS). Vesicular monoamine transporter 2 (VMAT2), which is responsible for monoamine (dopamine, norepinephrine, and serotonin) transport across synaptic vesicles, is implicated in tardive dyskinesias (TD) pathology.(48) Valbenazine (56), an inhibitor of VMAT2, was approved for the treatment of TD. Another VMAT2 inhibitor, deutetrabenazine (59), that depletes the levels of presynaptic dopamine was approved for the treatment of Huntington’s disease (HD).(49) Flibanserin (53), an agonist of 5-HTA1 and an antagonist of 5-HTA2, and bremelanotide (2019), a melanocortin receptor agonist, were approved for the treatment of hypoactive sexual desire disorder (HSDD) in premenopausal women. Histaminergic neurons play a significant role in the maintenance of wakefulness.(50) Pitolisant (66), a histamine H3 receptor antagonist or inverse agonist, was approved for the treatment of excessive daytime sleepiness (EDS) associated with narcolepsy in adults. Lemborexant (69) is a competitive antagonist of OX1 and OX2 receptors(51) and blocks the binding of neuropeptides orexin-A and -B. The drug suppresses the wake-drive, thereby promoting sleep, and is recommended for the treatment of insomnia. Nusinersen, an antisense oligonucleotide approved in 2016, increases the splicing efficiency of the SMN2 pre-mRNA and corrects the SMN protein deficiency involved in spinal muscular atrophy (SMA).
A total of 21 out of 23 small molecule drugs approved for various neurological disorders are intended for administration through the peroral route and 2 through the intravenous route. Three out of 4 monoclonal antibodies are approved for the subcutaneous route, and eptinezumab (a mAb, approved for migraine) was approved for administration through the intravenous route. Approved oligonucleotides are for intrathecal and subcutaneous administration.
CYPs played significant roles in the metabolism of 14 out of 23 small molecules, wherein the major enzyme involved is CYP3A4 (for 13 out of 14 approved drugs). Nucleases are involved in the metabolism of oligonucleotides, and catabolism continues to remain the primary way for elimination of the macromolecules. Seventeen small molecules were implicated as victims during coadministration with drugs causing modulations in enzymes (CYP3A4, CYP2C19, CYP2D6, and CYP1A2) and transporters (P-gp and BCRP). A majority of the approved small molecules followed the Lipinski’s rule of 5. By the end of 2020, ∼14% of the global population is anticipated to suffer from neurological disorders. Geographically, it is estimated that the largest market for neuro-therapeutics will be led by North America, followed by Europe and Asia-Pacific countries. The key players contributing to the market share will include Abbott, Becton and Dickinson, Novartis, Johnson & Johnson, Pfizer, Sanofi-Aventis, Biogen, GlaxoSmithKline, AstraZeneca, and Merck.(52)
Drugs for the Treatment of Metabolic/Genetic Disorders
Under this category, authors have observed that a total of 35 novel therapeutic agents were approved by the U.S. FDA in the specified period, with one-third of them being small molecules (12). Antibody molecules and oligonucleotides (4 each), peptides and enzymes (5 each), polymers, hormones (2 each), and one fusion protein constituted the remaining approvals. Considering the total 76 new molecular entities approved by the FDA for the treatment of metabolic disorders until 2015, the last 5 years seem to ensure that more number of drugs are available to the patients of metabolic disorders.(53) The details of all the drugs approved for metabolic disorders during the period 2015–June 2020 are compiled in Table, and chemical structures of small molecules are illustrated in Figure 5. A brief overview of the compilation is presented here. In the category of antihyperuricemic/antigout drugs, lesinurad (73), an URAT1(54) inhibitor which causes an increase in the excretion of uric acid, was approved. Patiromer, approved in 2015 for hyperkalemia, is a nonabsorbed potassium-binding polymer that binds to potassium in the gastrointestinal system, resulting in excretion of potassium in feces to reduce the serum potassium levels. Natpara (2015), a parathyroid hormone involved in regulating serum calcium levels, was approved for the treatment of hypocalcemia in adults with reduced PTH (parathyroid hormone) levels.(55) Incretins (glucagon-like peptide-1; GLP-1) are the hormones produced by the intestinal mucosa which regulate the insulin secretion in response to food consumption.(56) Lixisenatide (2016), a GLP-1 receptor agonist, and semaglutide (2017), a GLP-1 analogue, were approved for the management of type 2 diabetes mellitus. Another antidiabetic drug ertugliflozin (79) targeting SGLT2(57) was approved in 2017. Whereas for the treatment of type 1 diabetes, insulin degludec (2018), an ultralong-acting insulin analogue, was approved. Etelcalcetide (2017), a type 2 calcimimetic, is a positive allosteric modulator which increases the sensitivity of the calcium-sensing receptor (CaSR) to ionized calcium and reduces PTH secretion by the negative feedback mechanism. Pegvaliase, a recombinant phenylalanine ammonia lyase (PAL) enzyme which reduces blood phenylalanine concentrations by converting phenylalanine to ammonia and trans-cinnamic acid, was approved in 2018. Cushing syndrome is caused by chronic elevation of circulating glucocorticoids primarily by overproduction of cortisol by the adrenals as a result of a pituitary or adrenal tumor.(58) The preferred therapeutic strategy is to reverse hypercortisolemia. Osilodrostat (85), approved in 2020, is an inhibitor of 11β-hydroxylase, an enzyme involved in the biosynthesis of endogenous cortisol and results in reduced cortisol concentrations. Elevated extracellular levels of inorganic pyrophosphate (PPi) results in defective mineralization and leads to bone deformation in infants. Asfotase alfa (2015) treatment replaces the level of TN-SALP (tissue nonspecific alkaline phosphatase) enzyme and reduces the PPi levels. Eteplirsen (2016), is a targeted oligonucleotide that causes exon skipping of exon 51. Deflazacort (78), a corticosteroid was approved for the treatment of Duchenne muscular dystrophy. Cerliponase alfa (2017) contains tripeptidyl peptidase-1 (rhTPP1), a recombinant human lysosomal exopeptidase which cleaves the N-terminal of tripeptides. The drug was approved for the treatment of ceroid lipofuscinosis type 2 (CLN2). Vestronidase alfa (2017), a recombinant human lysosomal beta-glucuronidase (GUS) acts by serving as an exogenous source of GUS enzyme through intravenous infusion.(59) Migalastat (80), approved for the treatment of Fabry disease, stabilizes the dysfunctional alpha-Gal A enzyme and results in the clearance of accumulated crystalline glycosphingolipids (GSLs).(60) Increased levels of fibroblast growth factor 23 (FGF23) were observed in patients with X-linked hypophosphatemia (XLH).(61) Burosumab (2018) is a monoclonal antibody that inhibits the actions of FGF23, which in turn increases the tubular reabsorption of phosphate from the kidney. Voxelotor (81), an HbS polymerization inhibitor prevents the formation of abnormally shaped cells and was approved for sickle cell disease. In the same category, crizanlizumab (2019), an antibody targeting P-selectin was approved for the treatment of vaso-occlusive crisis in patients with sickle cell diseases. Luspatercept (2019), a fusion protein, ameliorates ineffective erythropoiesis in patients with beta thalassemia by acting as a “ligand trap” for various members of the TGF-β superfamily. Afamelanotide (2019), a synthetic analogue of the endogenous α-MSH, was approved to prevent skin damage in people with erythropoietic protoporphyria from UV-induced damage. Cystic fibrosis (CF) is a genetic disorder caused by mutations in the cystic fibrosis transmembrane conductance regulator (CFTR) gene which results in the production of abnormally thick mucus that builds up in the lungs, digestive tract, and other parts of the body.(62) There are more than 1700 different mutations in the CFTR gene that can cause CF, the most common one is the F508del (F: Phenylalanine) mutation. CFTR modulators are classified into potentiators (ivacaftor, 82), correctors (lumacaftor, 77 and tezacaftor, 84), and amplifiers (in clinical development; PTI - 428 and PTI - CH). Combination therapy is anticipated to offer better results than individual drug(s). Orkambi, symdeko, and trikafta are the three CFTR modulators approved during this period wherein orkambi and symdeko were approved for individuals with two copies of the F508del mutation (smaller CF population).(63) Trikafta (elexacaftor, tezacaftor and ivacaftor) is a triple combination therapy, which was approved for the treatment of CF patients with one or more F508del mutation in the CFTR gene (90% of the CF population). Going forward, the global CF market is expected to register a CAGR of 13.5% and is anticipated to reach USD ∼ 13 000 M by 2025.(64) Drug discovery efforts for CF are spearheaded by Vertex, AbbVie, Gilead, Actavis (Allergan), Genentech (Roche), and Novartis.
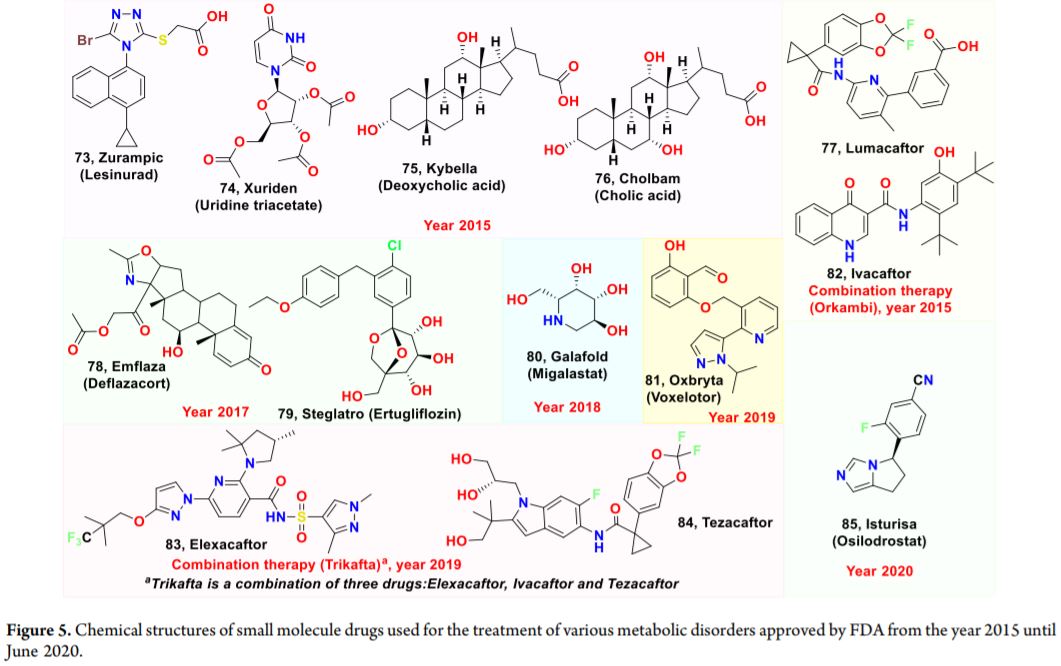
Figure 5. Chemical structures of small molecule drugs used for the treatment of various metabolic disorders approved by FDA from the year 2015 until June 2020.
Except for 77 and 83, all the approved small molecules under this category followed the Lipinski’s rule. As indicated in Table 4, some of the approved small molecules were implicated as victims during coadministration with drugs causing modulations in enzymes (CYP2C9, CYP2B6, and CYP3A4) and transporters (BSEP).(65) Eleven out of 12 small molecule drugs approved for various metabolic disorders are approved for administration through the peroral route and one through the subcutaneous route. Three out of 4 monoclonal antibodies are approved for use through the subcutaneous route, and crizanlizumab (monoclonal antibody, approved for sickle cell anemia to Novartis) was approved for the intravenous route. Oligonucleotides were approved through intravenous (3) and subcutaneous (1) administration. Two polymers are approved through peroral administration during this period for the treatment of hyperkalemia. Only 7 small molecules are metabolized through CYPs, wherein again the major enzyme involved is CYP3A4 (6 out of 7), and all these molecules behave as victims when codosed with CYP3A inducer/inhibitor. Dose adjustment is required for the drugs that are eliminated through the renal pathway (e.g., 78).
In 2017, the metabolic diseases market size was valued at ∼USD $50 billion, which is expected to rise at 7.6% of CAGR by 2024. Major contributing regions to research in this area and market for the therapies include Africa, North America, Asia Pacific, Latin America, the Middle East, and Europe. The notable companies involved in this area of research are GlaxoSmithKline, Merck, Amicus, Sanofi, Genzyme, AstraZeneca, and Horizon Pharma.(66) For genetic disorders, the market is expected to rise from USD $45 billion in 2017 to USD $86 billion by 2025. Important countries that will drive drug discovery in the area of genetic disorders are North America and the Asia Pacific region.
Drugs for Respiratory Disorders
Respiratory diseases including chronic obstructive pulmonary diseases (COPD), asthma, interstitial lung diseases, and pulmonary sarcoidosis(67) are the third leading cause of worldwide death.(68)
The U.S. FDA approved a total of just four drugs in the last five years for the treatment of asthma (3 mAbs) and chronic obstructive pulmonary disease (revefenacin 86, a small molecule). The details of the approved drugs for respiratory diseases are compiled in Table 5. The mAbs bind to the interleukin 5 receptor, a key cytokine responsible for the differentiation, maturation, recruitment, and activation of human eosinophils which plays a key role in inflammation associated with asthma. Mepolizumab and benralizumab have been approved by the FDA for administration through subcutaneous route, while reslizumab has been approved for use via the intravenous route. 86 is a bronchodilator, long acting muscarinic antagonist (LAMA), approved for dosing through the inhalation route. After inhalation, 86 rapidly undergoes hepatic metabolism to a major active metabolite (THRX-195518), with its systemic exposure being 4- to 6-fold greater than 86.(69) OATP1B1/1B3 inhibitors may increase serum concentrations of the active metabolite(s) of 86.(70)
There has been a recent upsurge in research in respiratory diseases’ drugs because of the Covid-19 pandemic, which primarily affects the respiratory system. The global market for drugs for respiratory diseases was estimated at $65 billion in 2019 and is expected to rise to $93 billion by end of 2020. North America accounted for 49% of the global market, followed by Western Europe (19%). Mylan, GlaxoSmithKline, AstraZeneca, Boehringer Ingelheim, Merck, Roche, Novartis, and Teva are considered to be key players that will drive the market for respiratory drugs.(71)
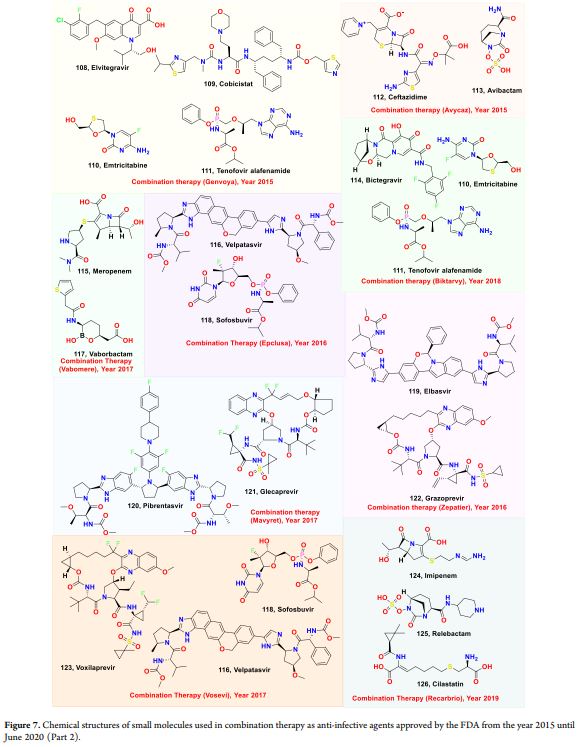
Anti-Infective Drugs
Infectious diseases are caused by pathogens, which include bacteria, fungi, protozoa, worms and viruses. There were 292 approved new molecular entities until late 2013 for the treatment of infectious diseases.(72) A total of 33 anti-infective drug/drug combinations were approved by US FDA in the last five years (Table 6 and Figure 6 and 7), with 90% being small molecules (30 drug/drug combinations) and 3 mAbs. The drugs approved for the various infectious diseases are briefly discussed with their targets in this section. Complicated urinary tract infections (cUTI) and complicated intra-abdominal infections (cIAI) are caused by multidrug-resistant bacteria.(73) Eravacycline 95,(2018), a synthetic fluorocycline antibiotic of the tetracycline, which binds to the 30S ribosomal subunit and disrupts bacterial protein synthesis was approved for the treatment of cIAI. Avycaz (the combination of ceftazidime 112, a cephalosporin antibiotic, and avibactam 113, a β-lactamase inhibitor, 2019), plazomicin 98, an aminoglycoside which targets bacterial 30S ribosomal subunit and cefiderocol 103, an inhibitor of penicillin-binding proteins (PBPs) were approved for treatment of cUTI. Vabomere, is a combination of Meropenem 115, a penam antibacterial, and vaborbactam 117, a beta-lactamase inhibitor was approved in 2017 for the treatment of patients with cUTI. Recarbio is a combination of imipenem 124, a carbapenem antibacterial, cilastatin 126, a renal dehydropeptidase inhibitor, and relebactam 125, a beta-lactamase inhibitor. The combination prevents the degradation of 124 by serine beta-lactamases. Recarbio was approved for the treatment of cIAI and cUTI in 2019. In 2020, the drug is also approved for the treatment of hospital-acquired bacterial pneumonia and ventilator-associated bacterial pneumonia. Lefamulin (104), which exerts its action by binding to the peptidyl transferase center of the ribosomal bacterial 50S subunit and omadacycline (99), a minomethylcycline subclass of tetracycline antibiotics were approved for the treatment of community-acquired bacterial pneumonia (CABP). Tuberculosis, which is estimated to infect one in every three people is caused by Mycobacterium tuberculosis.(74) Pretomanid (106) is indicated for the treatment of pulmonary forms of nonresponsive multidrug-resistant (MDR) tuberculosis, in combination with bedaquiline and linezolid.(75)
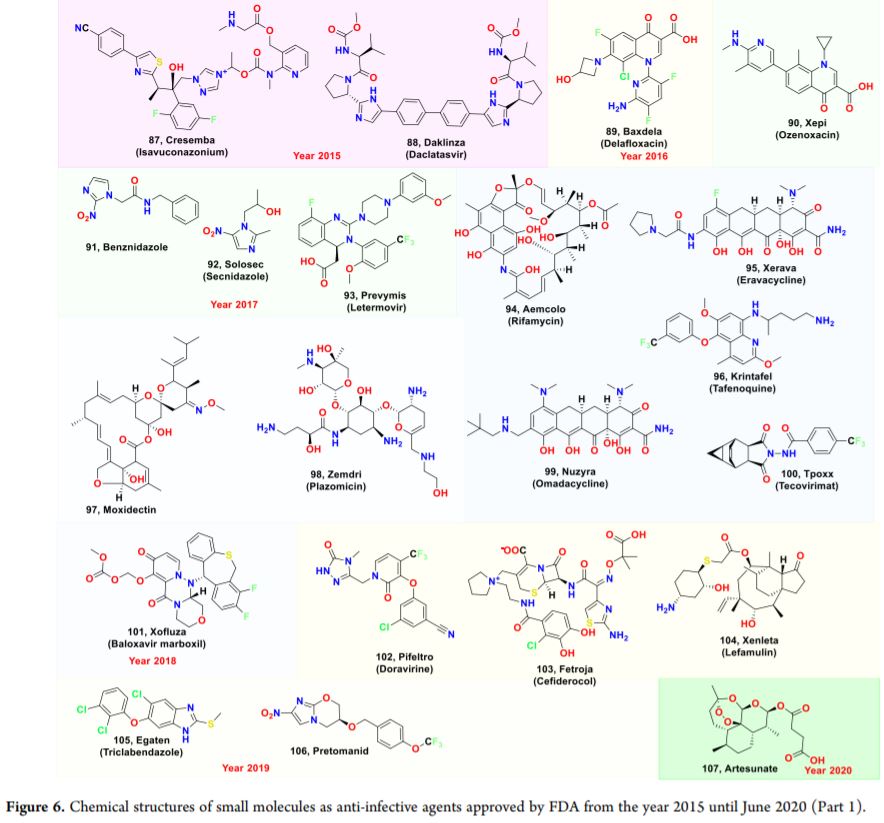
Delafloxacin (89), an anionic fluoroquinolone, which inhibits the activity of bacterial topoisomerase II was approved in 2017 for the treatment of acute bacterial skin and skin structure infections caused by Staphylococcus, Enterococcus, Escherichia coli, Klebsiella pneumoniae, and Pseudomonas aeruginosa.(76) Ozenoxacin (90), which targets bacterial DNA replication enzymes DNA gyrase A and topoisomerase IV was approved in 2017 for the topical treatment of impetigo. Secnidazole (92), a second-generation 5-nitroimidazole was approved in 2017 for the treatment of bacterial vaginosis in adult women.(77) In 2016, two mAbs, bezlotoxumab for Clostridium difficile infection(78) and obiltoxaximab for the prevention and treatment of infection caused by anthrax toxin were approved.(78) Further analysis revealed that three small molecules and one mAb were approved in the anti-HIV category. The approved small molecules, in general, were combination drugs which target HIV-1 integrase strand transfer (involves in concerted integration of viral DNA into the host chromosomes), nucleoside and nucleotide reverse transcriptase (reverse transcribes viral RNA into DNA for insertion into the host DNA sequence). An anti-HIV mAb, Ibalizumab which, targets CD4 receptors on the surface of CD4-positive cells and prevent HIV particle entry into the lymphocytes was approved in 2018. Influenza is an acute respiratory disease caused by the influenza A or B virus with an annual incidence of 3–5 million cases of severe illness and about 250,000 to 500,000 deaths worldwide.(79) Baloxavir marboxil (101), a prodrug, the hydrolysis of which results in baloxavir, is responsible for activity against influenza A and B virus infection. 101 exerts its activity by selectively inhibiting influenza cap-dependent endonuclease which prevents polymerase function leading to influenza virus mRNA replication. 101 is the only new flu drug to be approved since the 1999 approval of Roche’s neuraminidase inhibitor oseltamivir.
Hepatitis C virus (HCV), belonging to family Hepadnaviridae, affects around 170 million people worldwide.(80) Five single and/or combination of small-molecule drugs were approved for the treatment of HCV between 2015 - June 2020. Most of the approved drugs target HCV nonstructural protein 5B (NS5B), the RNA-dependent RNA polymerase responsible for the complete copy of the RNA viral genome, HCV nonstructural 5A (NS5A) protein involved in modulation of the host cell interferon (IFN) response and HCV NS3/4A protein, a membrane-targeted serine protease responsible for maturation of the viral polyprotein.(81)
Cytomegalovirus and smallpox infections are caused by β-herpesvirus (HHV-5) and variola virus, respectively. Letermovir (93) inhibits the activity of the DNA terminase complex of cytomegalovirus (CMV) and was approved for prophylactic treatment of CMV infection in allogeneic hematopoietic stem cell transplant patients. Tecovirimat (100), an inhibitor of the orthopoxvirus VP37 envelope wrapping protein was approved for the treatment of smallpox.(82) As per the World Malaria Report 2018, there were 219 million cases of malaria globally in 2017 with around 4,35,000 malaria deaths.(83) Artesunate 107, (2020) was approved for the treatment of severe malaria and it generates free radicals that inhibit the normal function of Plasmodium parasites. Tafenoquine (96), an 8-aminoquinoline analogue of primaquine which acts through its active moiety 5,6-orthoquinone tafenoquine generates hydrogen peroxide and hydroxyl radicals which further causes the parasitic death.(84) Benznidazole (91) was approved in 2017 for the treatment of Chagas disease caused by Trypanosoma cruzi in children. For triclabendazole (105), the mechanism of action is not fully known and is currently the only FDA-approved drug for patients affected with fascioliasis. It is postulated to inhibit tubulin function and synthesis of proteins and enzymes in the parasite. Onchocerciasis (river blindness) is caused by a nematode worm, Onchorcerca volvulus. Moxidectin (2018) which binds to the parasite’s GABA-A and glutamate-gated chloride ion channels was approved for the treatment of river blindness. Isavuconazonium (87), a second-generation triazole antifungal inhibits the sterol 14-α-demethylase (Erg11p), and thereby disrupts the fungal membrane integrity. 87 was approved in the year 2015 by the FDA for the treatment of invasive aspergillosis and invasive mucormycosis.
Majority of the drugs in this category were proved for the treatment of bacterial and viral infections. Agreement to Lipinski’s criteria for majority of the approved small molecules (27) continued to be the case with anti-infective drugs. A total of 16 small molecules are metabolized through CYPs, wherein major enzyme involved is CYP3A4 (14 out of 16) and behave as victims when codosed with CYP3A inducer/inhibitor. For ∼70% of the small molecule drugs, peroral route has been approved for administration and 8 drugs are approved for use through intravenous route.
The global market size of anti-infectious agents was valued at ∼ USD 47 billion in the year 2016. The market can be broadly segmented into HIV, malaria, hepatitis, influenza, human Papillomavirus and tuberculosis. In 2016, the HIV segment held the largest share followed by hepatitis therapeutics segment.(85) The major pharmaceutical companies dominating anti-infective drug development include Merck & Co., F. Hoffmann-La Roche Ltd., Pfizer, Johnson & Johnson Services and GlaxoSmithKline.(86)
Drugs for Autoimmune Disorders
Autoimmune diseases comprise more than 70 different disorders affecting approximately 5% of the general population.(87) The autoimmune disorders are reported to be among the 10 most frequent underlying or contributory causes of mortality in females (women have increased prevalence of autoimmune diseases as compared with men) of all age groups with the peak mortality rate of ∼5% between 55 and 74 years.(88)
Unitl 2014, there were a total of 168 new molecular entities approved for the treatment of autoimmune diseases.(89) In the last five years, the FDA approved a total of 25 therapeutic agents with a majority of them being mAbs (14 drugs) and one enzyme, while small molecules contributed toward approval of 10 drugs (Table 7 and Figure 8).
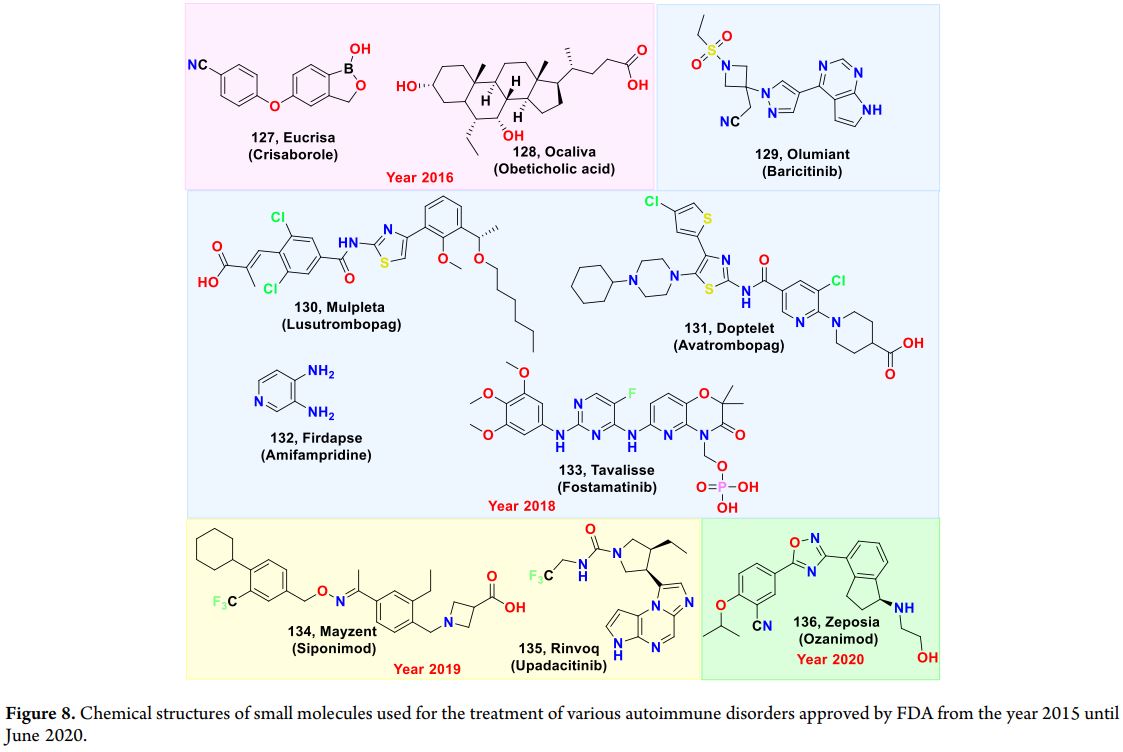
Multiple sclerosis (MS) is a chronic inflammatory disease of the central nervous system (CNS).(90) Drugs modulating sphingosine-1-phosphate (S1P) receptors, interleukin-2 (IL-2) receptor, and CD-20 on B lymphocytes were approved for MS in the period of study. The S1P1 receptor family comprises five members with effects on cell proliferation, migration and survival, intercellular communication, vascular tone, and endothelial barrier function.(91) Two small-molecule modulators, siponimod 134 (S1P1) and ozanimod 136 (S1P1 and S1P5), were approved for MS in 2019 and 2020, respectively. Further, in addition to T lymphocytes, B lymphocytes could also produce pro-inflammatory cytokines in MS. Ocrelizumab (2017), a second-generation recombinant humanized monoclonal IgG1 antibody that selectively targets the B lymphocytes which express the CD20 antigen was approved for MS.(92) Interleukin-2 (IL-2) and its receptor play a key role in the proliferation of autoreactive T cells and loss of immune tolerance in MS. Considering this rationale, daclizumab (2016), a humanized mAb that binds to CD25, the alpha subunit of IL-2 receptors was approved for the relapsing forms of MS. However, the drug was withdrawn from the market in March 2018 due to safety concerns involving inflammatory brain disorders in patients.(93) Atopic dermatitis (AD) is a chronic inflammatory skin disease characterized by strong itching resulting from amplified immune response to environmental pollutants and toxins.(94) The prevalence of AD is reported to be 10.7% in children in the United States.(95) The amplified immune response is mediated by interleukin (IL)-4 signaling through IL-4 receptor alpha (IL4Rα), which also mediates IL-13 signaling.(96) Dupilumab (2017) acts against the interleukin-4 receptor subunit α (IL-4Rα) of IL-4 and IL-13 receptors. The phosphodiesterase 4 (PDE4) enzyme is responsible for inflammatory cytokine production. Crisaborole (127), a novel PDE4 inhibitor, was approved by the FDA in 2016 through the topical route for the treatment of moderate AD. Interleukin-23 is a key cytokine connecting the innate and adaptive components of the immune response.(97) Elevated levels of IL-23 are related to several autoimmune diseases including rheumatoid arthritis and psoriasis.(98) The worldwide prevalence of psoriasis is reported to be up to 11.43% in adults. Guselkumab (2017) and risankizumab (2018) are IL-23 antagonists and were approved for the treatment of patients with moderate-to-severe psoriasis for administration through the subcutaneous route. Th17 cells are the subset of helper T cells and are reported to play a major role in the pathology of multiple autoimmune diseases through the production of interleukin-17. Blocking of the Th17 axis, either by inhibition of IL-17 directly or by intercepting Th17 cell differentiation, was considered as one of the therapeutic strategies.(99) Three IL-17A antagonists, namely, ixekizumab, secukinumab, and brodalumab, were approved for treatment of psoriasis in the period of study. Interleukin-6 (IL-6) is reported to be present in higher levels in both the synovium and serum of rheumatic arthritis (RA) patients.(100) The worldwide prevalence of RA was reported to be 0.25%.(101) Sarilumab (2017), an IL-6 receptor antagonist binds to soluble as well as membrane-bound IL-6 receptors (sIL-6R and mIL-6R) and was approved for the treatment of adult patients with moderately to severely active RA. JAKs (intracellular tyrosine kinases) play a significant role in cytokine signaling pathways involving immunity and hematopoiesis.(102) The different types of JAKs identified are JAK1, JAK2, JAK3, and tyrosine kinase 2 (TYK2). JAK signaling inhibition offers a novel mechanism through which a range of cytokines can be inhibited using a small-molecule drug. Tofacitinib (a first-generation JAK inhibitor) is a pan-JAK inhibitor having the ability of inhibiting JAK3/1/2 and to a minor extent TYK2, and it was approved for the treatment of RA. Baricitinib (129), a selective JAK1 and JAK2 inhibitor, was approved for the treatment of RA in 2018.(103) Recently, second-generation JAK inhibitors that exert a selective inhibition of JAK1 or JAK3 have been explored.(104) Upadacitinib (135) is an oral JAK1-selective inhibitor, with a negligible effect on JAK3, leading to an improved drug safety profile. 135 was approved for the treatment of RA in August 2019.(105) Thrombocytopenia is the most common hematologic complication in patients with chronic liver disease defined by a platelet count below 150 000/μL. The prevalence of thrombocytopenia in patients with chronic hepatitis was reported to be 6%; however, a prevalence of up to 78% was reported in cirrhotic patients.(106)Immune thrombocytopenia (ITP) is identified by immune-mediated destruction of platelets which results in thrombocytopenia and mucocutaneous bleeding. Thrombopoietin receptor agonists belong to a class of platelet growth factors that mimic the action of endogenous thrombopoietin (TPO) on megakaryocytes and their precursors leading to promotion of their growth and differentiation and thereby increasing platelet production.(107) Avatrombopag (131) and lusutrombopag (130) were approved in May and July 2018, respectively, for the treatment of thrombocytopenia as a result of chronic liver disease. Fostamatinib (133) is a small-molecule inhibitor of spleen tyrosine kinase (Syk) and was approved in the year 2018 for the treatment of ITP.(108) Upregulation of FNγ leads to hemophagocytic lymphohistiocytosis (HLH).(109) Emapalumab, a monoclonal antibody that binds to and neutralizes interferon gamma (IFNγ), was approved in the year 2017 for the treatment of primary HLH in patients. Paroxysmal nocturnal hemoglobinuria (PNH) is a rare acquired condition resulting from defective synthesis of GPI-anchored proteins due to a somatic mutation in the Pig-A gene in bone marrow stem cells.(110,118) The true incidence of PNH is unknown, but it was estimated at 1.5–2.0 cases per million of the population per year.(111) Ravulizumab was approved in 2018 for the treatment of PNH. Ravulizumab binds to complement protein 5 (C5) and blocks its activation by complement pathway convertases, thus inhibiting the formation of the terminal complement complex.(112) Lambert-Eaton myasthenic syndrome (LEMS) is a neuromuscular junction disorder that is characterized by the presence of autoantibodies against P/Q type voltage-gated calcium channels, which results in improper release of acetylcholine at presynaptic membrane.(113) The estimated global prevalence of LEMS is about 2.8 per million. Amifampridine, approved in 2018, is a symptomatic treatment that increases acetylcholine concentrations at the neuromuscular junction. Adenosine deaminase (ADA) is an important enzyme involved in the purine salvage pathway.(114) Mutation of the ADA gene results in accumulation of toxic metabolites such as adenosine, 2’deoxyadenosine, and deoxyadenosine triphosphate, which further results in a form of severe combined immunodeficiency (SCID) characterized by severe lymphocytopenia and NK cells.(115) Adenosine deaminase deficiency is very rare with the global incidence of approximately 1 in 200 000 to 1 000 000 newborns.(116) Elapegademase has the ability to increase adenosine deaminase activity while reducing the concentrations of toxic metabolites and was approved in 2018.(117) Primary biliary cholangitis (PBC) is an autoimmune liver disease, characterized by biliary destruction, progressive cholestasis, and liver damage.(118) Farnesoid X Receptor (FXR) is a bile acid receptor, and its activation controls enterohepatic bile acid homeostasis, inflammation, and fibrosis in response to liver injury.(119) Obeticholic acid (128), a FXR agonist, was approved in 2016 for the treatment of PBC.(120) Thyroid eye disease (TED) is an autoimmune disease resulting in permanent facial deformity. Teprotumumab (2020), directed against IGF-1R (insulin-like growth factor-1 receptor), causes internalization and degradation of IGF-1R, which results in ameliorating the symptoms of thyroid eye disease.
Interestingly, 80% of the approved small molecules (8 out of 10) for the treatment of autoimmune disorders followed Lipinski’s rule. Half of the drugs (5 out of 10) were implicated as victims when coadministered with drugs causing modulations in enzymes (CYP3A4, CYP2C9, and CYP2C8) and transporters (BCRP and OAT3). Nine out of 10 small molecule drugs are approved for use through the peroral route and only one drug is approved through the topical route. Five mAbs are approved for administration through the intravenous route, and nine are approved for use through the subcutaneous route. The key players currently involved in discovery and development of drugs for autoimmune diseases are AbbVie, Trinity Biotech, Biorad Laboratories, F. Hoffmann-la Roche, Inova Diagnostics along with Johnson & Johnson, Eli Lilly & Co., Bristol Myers Squibb, Abbott Laboratories, Pfizer, and AstraZeneca.(121)
Cardiovascular Drugs
A report from the WHO (2019) indicated that cardiovascular diseases (CVDs) result in a mortality of 17.9 million (31% of all deaths worldwide) globally.(122) The CVDs include cerebrovascular disease, deep vein thrombosis, coronary heart disease, rheumatic heart disease, peripheral arterial disease, congenital heart disease, and pulmonary embolism. Among the CVDs, heart attacks and strokes are primarily responsible for the mortality.(123) From the period of 1937– 2013, there were 201 new molecular entities approved for treatment of CVDs.(124) During the last five years, a total of 15 therapeutic agents for CVDs were approved by US FDA, with a majority of them being small molecules (9 drugs), while macromolecules constituted the remaining (Table 8 and Figure 9). The drugs approved under this category are described subsequently.
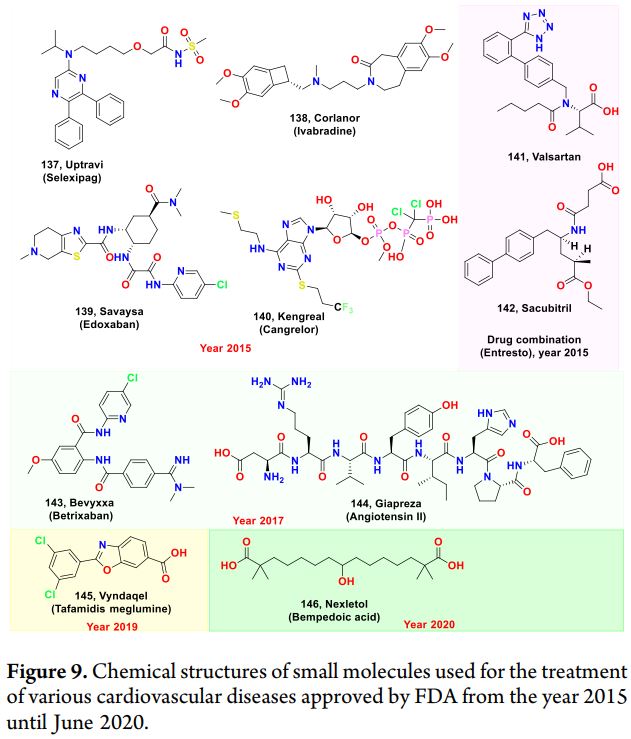
A drug combination comprising of sacubitril (142) and valsartan (141) was approved in 2015 for the treatment of chronic heart failure.(125) The combination is based on the inhibition of neprilysin by active metabolite of 142, LBQ657, which in turn increases the bioavailability of brain natriuretic peptide (BNP), atrial natriuretic peptide (ANP), and c-type natriuretic peptide (CNP), which promote vasodilation, while the antihypertensive effect of 141 was mediated by its selective binding to angiotensin receptor 1 (AT1) and prevents angiotensin II from binding. Ivabradine was approved in 2015 for the management of symptomatic chronic heart failure for its heart rate lowering effect mediated by inhibition of the cardiac pacemaker current, a mixed sodium–potassium inward current. Proprotein convertase subtilisin/kexin type 9 (PCSK9) is reported to play a major role in cholesterol metabolism, by reducing the expression of the LDL receptor.(126) Nonvitamin K antagonist oral anticoagulants (NOACs) are preferred because of their selective action, shorter half-life, and safety.(127) Edoxaban (139) exerts its action by inhibiting factor Xa (FXa), an important component of the coagulation cascade, and it was approved in 2015 for reducing the risk of embolism. Selexipag (137), a selective prostacyclin receptor agonist, was approved for the treatment of pulmonary arterial hypertension. Inhibition of PCSK9 results in increased LDL cholesterol receptors with the decrease in serum LDL cholesterol.(128) Two monoclonal antibodies alirocumab and evolocumab targeting PCSK9 were approved in 2015 for the treatment of hypercholesterolemia. Considering the role of Angiotensin II by causing vasoconstriction with a resultant increase in blood pressure, first synthetic human Angiotensin II was approved in 2017 for increasing blood pressure in patients with septic shock.(129) Emicizumab, which mimics the function of the coagulation Factor VIII, was approved in 2017 as a prophylaxis to prevent the frequency of episodes of bleeding patients with hemophilia A. Tafamidis (145), a transthyretin stabilizer, was approved in 2019 to treat cardiomyopathy caused by transthyretin-mediated amyloidosis.(130) Caplacizumab, approved in 2019 for the treatment of thrombotic thrombocytopenic purpura in conjunction with plasma exchange, acts by targeting the A1 domain of the ultralarge von Willebrand factor and prevents the interaction between the von Willebrand factor and platelet aggregation.
Almost all approved small molecules (8 out of 9) in this category followed Lipinski’s rule. Data in Table 8 show that some of the approved drugs (small molecule) were implicated as victims during coadministration with other drugs causing modulations in enzymes (CYP2C8 and CYP3A4) and transporters (P-glycoprotein). The major route of administration for small molecules cardiovascular drugs continues to be the peroral one, and only two drugs are approved for use through the intravenous route. Five monoclonal antibodies are approved through the subcutaneous route, and one is approved for administration through the intravenous route. Catabolism is primarily responsible for the elimination of all the macromolecules. The cardiovascular drugs market is expected to be dominated by North America, the United States, Canada, the U.K., and Europe (Germany, Spain, Italy, and France). The pharmaceutical companies such as Bristol Myers Squibb, Abbott, AstraZeneca, Takeda, Novartis, Bayer, Roche, GlaxoSmithKline, Daiichi Sankyo, Pfizer, Johnson & Johnson, and Solvay SA are currently researching the discovery and development of novel drugs for cardiovascular diseases. The rise in diabetic patients also holds a potential role in elevating the global cardiovascular drugs market, which is already hampered by stringent regulations and patent expiry of numerous blockbuster drugs in near future.(131)
Diagnostic Agents
Diagnostic agents are primarily used to aid in detecting abnormalities at cellular and molecular levels.(132,133) These agents should possess high quantum yield (sensitive) and photostability and should be expeditious to cross the cell membrane with low or no cytotoxicity at a concentration of investigation.(134) In the late 19th century, fluorescein and rhodamine derivatives were first reported as diagnostic agents for bioimaging.(135) The meagre photostability of these dyes restricts their application in bioimaging applications, where prolonged illumination is essential.(136) Therefore, de novo design and development of a safe, quick, and effective diagnostic agent continues to be a prominent area of research.(137)
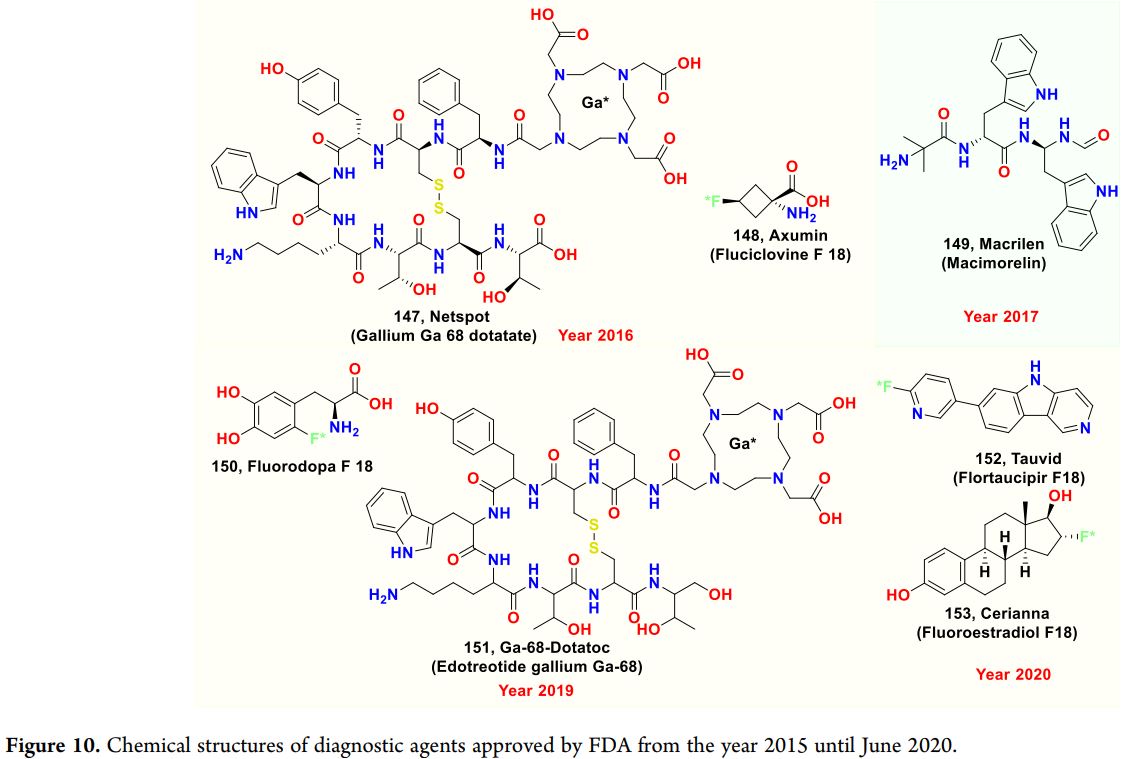
In the last five years, the FDA has approved eight diagnostic agents (seven small molecules and one polymer). Fluciclovine F18 (148), fluorodopa F18 (150), flortaucipir F18 (152), and fluoroestradiol F18 (153) are approved for the diagnosis of prostate cancer, Parkinsonian syndrome, Alzheimer’s disease, and breast cancer, respectively. Two gallium-containing radioactive diagnostic agents (147 and 151) have been approved for the diagnosis of a neuroendocrine tumor. A general mechanism behind these diagnostic agents lies in their uptake through the targeted receptors present on the diseased organ; for example, uptake of 148 will increase through L-type amino acid transporter (LAT) receptors present on the prostate cancer cell. The details of the approved drugs are compiled in Table 9, and chemical structures are illustrated in Figure 10. A majority (6 out of 7) of small-molecule diagnostic agents are approved for use through the intravenous route, and only one is approved through the peroral route. One polymer (Giskit) was approved in 2019 through the intrauterine route for diagnosing fallopian tube patency.
According to the recent market trends, the global market for the imaging/diagnostic agents is expected to rise to $2.5 billion USD by 2024 at a CAGR of roughly 3.1%. The diagnostic radiopharmaceuticals are expected to grow at a rate of 3.5% with the market to rise to $6.4 billion USD.(138) The major global market includes the United States, Europe, and Germany. Aytu BioScience, Bayers Health Care, Bracco Diagnostic Inc., Curium, and Eli Lilly will be emerging key players.(139)
Miscellaneous Drugs
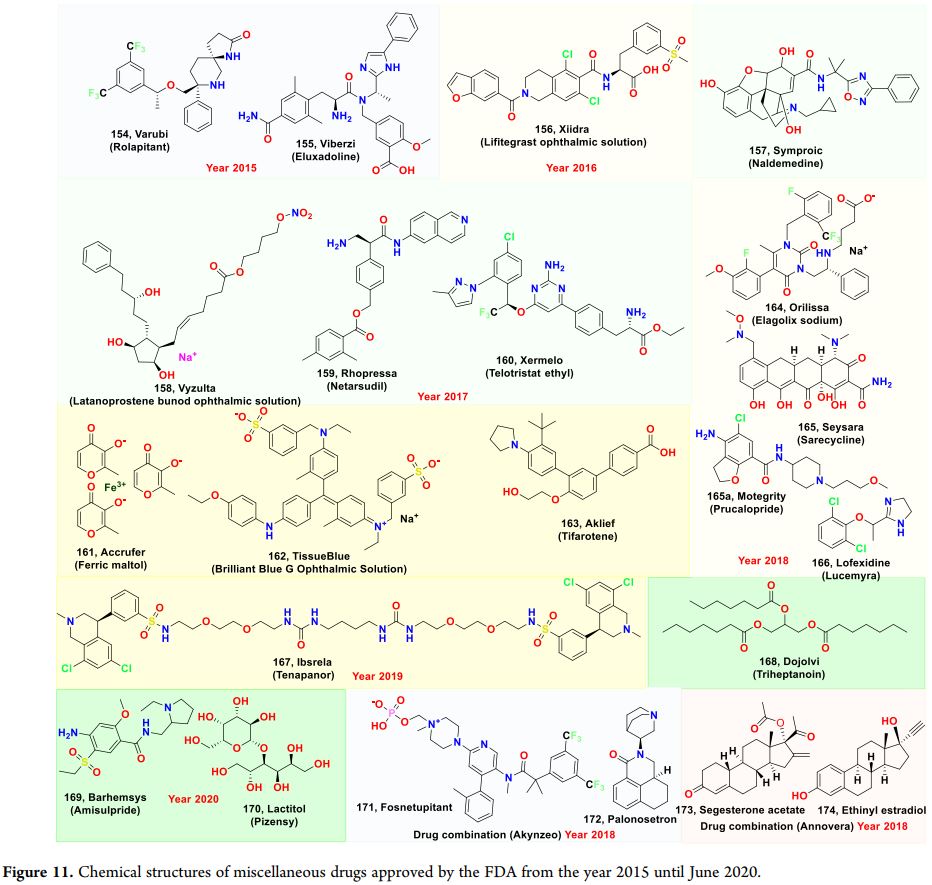
Drugs which could not be classified under any of the disease areas discussed in this review are reported under this category (<10% of the total number of approvals). A total of 25 drugs were approved by the FDA in the last five years (20 small molecules, 2 peptides, and 3 macromolecules). These can be further categorized into drugs for ophthalmic disorders (6 drugs), gastrointestinal diseases (10 drugs), reproductive disorder (3 drugs), dermatology (2 drugs), opioid withdrawal (1 drug), and nutrition supplements (3 drugs). The drugs approved under these categories are briefly discussed in this section (see Table 10 and Figure 11).
Ophthalmology
The leading causes of blindness and low vision are primarily diseases such as age-related macular degeneration (AMD), cataract, diabetic retinopathy, and glaucoma.(140) The global prevalence of vision impairment or blindness is around 2.2 billion. Latanoprostene bunod (158, a prostaglandin analogue) and Netardusil (159) are a Rho kinase and a norepinephrine transporter inhibitor, respectively, approved by the FDA in 2017 for patients with glaucoma or ocular hypertension through reduction of intraocular pressure (IOP). Lifitegrast 156 (the first lymphocyte function-associated antigen-1 antagonist) is indicated for the treatment of dry eye disease.(141) Two macromolecules, cenegermin (human nerve growth factor; 2018) and brolucizumab (human VEGF inhibitor; 2019) were approved for the treatment of neurotropic keratitis and wet AMD, respectively.
Gastrointestinal Disorders
Nausea/vomiting, constipation, and irritable bowel syndrome (IBS) broadly constitute functional gastrointestinal disorders (FGID) and are the three conditions for which nine new molecular entities were approved from the year 2015 until June 2020. FGID are reported to cause a serious reduction in the quality of life of people, which in turn put a huge impact on health care worldwide.(142) Discovering drugs for treating FGID are challenging as these are complex conditions, and the pathophysiology is affected by multiple factors including genetic predispositions, infection, chronic stress, and psychological symptoms.(143) Drugs approved for nausea and vomiting in this period are rolapitant (154) and amisulpride (169), which act as substance P/NK1 receptor antagonist and D2 antagonist, respectively. Chemotherapy-induced nausea and vomiting (CINV) is the most devastating side effect of chemotherapy in cancer patients.(144) Akynzeo, a combination of fosnetupitant (171) and palonosetron (172), was approved in 2018 through the intravenous route by the FDA because of its ability to prevent both nausea and vomiting associated with cancer chemotherapy. Irritable bowel syndrome (IBS) affects the large intestine, which results in diarrhea or constipation or both.(145) Eluxadoline (155) is a mixed opioid receptor agonist (Mu) and antagonist (delta) used for treating patients with diarrhea-predominant IBS.(146) Another drug, tenapanor (167), was the first sodium/hydrogen exchanger isoform 3 (NHE3) transporter inhibitor. It was approved for the treatment of constipation-predominant irritable bowel syndrome (IBS-C). Chronic idiopathic constipation (CIC) accounts for the global prevalence of 14% and is more common in women.(147) Three drugs, namely, plecanatide, prucalopride, and lactitol, were introduced into the market for CIC in this period. Plecanatide and lactitol (170) accelerate GI transit through the increased intestinal fluid.(148) Prucalopride (165a) is a selective 5-HT4 stimulator in the GI tract and increases intestinal motility by releasing acetylcholine.(149) The main advantage of prucalopride is that it has no interaction with the hERG channel or 5-HT1 receptors, which further reduces the cardiovascular risk. Opioids are known to cause constipation through inhibition of gastric emptying and peristalsis.(150) By antagonizing opioid receptors, naldemedine (157) inhibits opioid-induced constipation.(151) The tryptophan hydroxylase inhibitor xermelo (160) was approved for the treatment of carcinoid syndrome diarrhea in the year 2017.
The key players of global gastrointestinal drugs market are Takeda Pharmaceuticals, Allergan Plc, Novo Nordisk, AstraZeneca Plc, and AbbVie.(152)
Nutrition Supplements
Iron deficiency is one of the most common nutritional disorders prevalent in women and children that could result in restless legs syndrome (RLS), impaired cognitive function, fatigue, diminished quality of life, and infertility.(153) Accrufer (161; ferric maltol), approved in July 2019, is a novel, stable, nonsalt-based oral treatment for adults with iron deficiency. A calorie supplement (fish oil triglycerides and triheptanoin) was also approved in this study period.
Dermatology
Acne vulgaris is the inflammatory disease characterized by the formation of pustules, comedones, nodules, cysts, and/or papules, due to obstruction and inflammation of pilosebaceous units.(154) The market size of global acne drugs was around USD $4.1 billion in 2017. Two small-molecule drugs, sarecycline (165) and tifarotene (163), were approved by the FDA for acne vulgaris treatment during the study period.
Reproductive Disorders
Annovera (a combination of segesterone acetate 173 and ethinyl estradiol 174) was approved for the prevention of pregnancy in 2018.(155) Elagolix sodium (2018), a GnRH receptor antagonist, which reduces the levels of estrogen, was approved for the management of pain associated with endometriosis.(156)
Around 70% of the approved small molecules under the miscellaneous category (14 out of 20) followed Lipinski’s rule of 5. Evaluation of DDI data of these drugs revealed a majority of them are classified as victims (5 out of 20) when dosed along with CYP3A inhibitors and inducers. Three drugs are classified as perpetrators based on their role of the substrate to P-gp, OATP1B1, and BCRP.
Analysis of Approved Drugs
As per a report by the Global Burden of Disease (WHO), noncommunicable diseases are expected to be responsible for 7 out of 10 deaths in developing nations. Further, stroke, cardiovascular, respiratory, and neurological disorders along with cancer are the major causes of mortality worldwide. In line with the trend of anticancer drugs leading the total number of approvals, the highest number of approved drugs in any single year was also for this dreaded disease (i.e., 16 in the year 2018). Neurological disorders with high unmet medical need accorded the next spot with 11 approvals in the year 2019. Further, considering the ongoing viral pandemic due to Covid-19, drug approvals for infectious and respiratory diseases are expected to rise along with more immunotherapies coming into the market in the foreseeable future.
While the focus of research on large molecules is steadily increasing across the pharmaceutical industry and the number of approvals in this area have increased, the data suggest that during the study period, more than 2/3rd of the approved drugs were small molecules. Approvals for TIDES that include peptides and nucleotides have also increased in the past five years or so, and overall, their contribution is ∼10% of the total approvals. Among the macromolecules, the major share has been taken by mAbs followed by enzymes and oligonucleotides. Most of the biologics have been approved for the treatment of cancer followed by autoimmune and cardiovascular diseases.
An interesting observed trend during the study period was the increased number of approvals with the pricier “orphan drug” tag, which are used for the treatment, prevention, or diagnosis of a rare disease. Until 2015, a total of 281 orphan drugs were approved, consisting primarily of biologics (60%). The number of “orphan drug” approvals during the last five years (total approvals: 106) have almost doubled compared with the preceding five years, that is, 2010–2014 (total approvals: 56). Figure 12 illustrates orphan status versus the total number of approved drugs for different therapeutic areas during the study period. Cancer and metabolic disorders had the maximum number and pe
Copyright© Shanghai VastPro Technology Development Co., Ltd. 2016-2019 Supported by ChinaChemNet Toocle Copyright Notice
4th Floor, Building 9B, 100 Haike Road, Pudong New Area District, Shanghai, 201210 P. R, China.
Tel: +86-21-20608178 Fax: +86-21-20608171 Contact us


